|
Most cases of tennis elbow can be successfully treated with rest, bracing, ice, anti-inflammatory medication and corticosteroid injection. Recovery can be slow and recurrence may occur. When symptoms do not respond to conservative management, surgery is performed. Through a small incision, degenerated tendon tissue is (cleaned out) and the underlying bone is drilled to create bleeding which is necessary for tendon repair. Most patients achieve pain relief and are able to return to sports participation in 3 months. |
 |
|
|
Carpal tunnel syndrome is a common source of hand numbness and pain. The tendons in the wrist swell and put pressure on the , one of three major nerves responsible for supplying feeling in the hand. It is more common in women than men and affects up to 10 percent of the entire population. |
 |
||
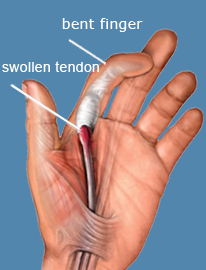
Trigger finger, or, is a condition in which the tendons that flex the fingers become swollen and inflamed. This results in pain at the base of one or more of the fingers. Locking or triggering of the finger frequently occurs as the swollen tendon tries to slide through the narrow tunnel that begins where the finger attaches to the palm of the hand. Symptoms frequently respond to corticosteroid injection. When they do not, outpatient surgery is very effective in relieving these symptoms. Under local anesthesia, a ½ inch incision is created to access the tendon and its tunnel. The entrance to the tunnel is divided, relieving pressure on the tendon, eliminating pain and locking. |
|
 |

Elbow / Wrist / Hand